Unmasking The Culprit – Pseudoaneurysm of Petrous Internal Carotid Artery
Anju KR1*, Swapna UP2, Nikhila R3, Anjali V4
DOI:https://doi.org/10.17511/ijmrr.2025.i02.07
1* Anju Krishna R, Junior Resident, Department of ENT, Sree Uthradom Thirunal Academy of Medical Sciences, Vattappara, Trivandrum, Kerala, India.
2 Swapna UP, Professor and HOD, Department of ENT, Sree Uthradom Thirunal Academy of Medical Sciences, Vattappara, Trivandrum, Kerala, India.
3 Nikhila Rajendran, Assistant Professor, Department of ENT, Sree Uthradom Thirunal Academy of Medical Sciences, Vattappara, Trivandrum, Kerala, India.
4 Anjali Vinod, Assistant Professor, Department of ENT, Sree Uthradom Thirunal Academy of Medical Sciences, Vattappara, Trivandrum, Kerala, India.
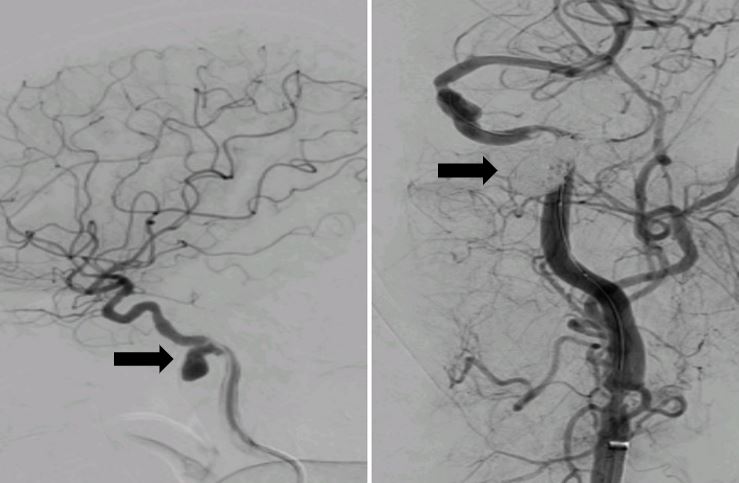
Pseudoaneurysms of the petrous internal carotid artery are rare. This is the case of a patient who presented with intermittent episodes of profuse bleeding from the left nostril and pulsatile tinnitus. Digital subtraction angiography (DSA) showed a pseudoaneurysm from the left petrous internal carotid artery which was promptly treated with balloon-assisted coiling.
Keywords: Pseudoaneurysm, epistaxis, internal carotid artery, balloon occlusion test, endovascular coiling
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Junior Resident, Department of ENT, Sree Uthradom Thirunal Academy of Medical Sciences, Vattappara, Trivandrum, Kerala, India. Email:  |
Anju KR, Swapna UP, Nikhila R, Anjali V, Unmasking The Culprit – Pseudoaneurysm of Petrous Internal Carotid Artery. Int J Med Res Rev. 2025;13(2):34-36. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1545 |
 |
 ©
©