Small bowel obstruction in Peutz-Jeghers syndrome: case report
Abdelhak E1, Khalid J2, Mosaab E3*, Khadija K4, Abdessamad M5, Mounir B6, Abdelilah E7, Khalid E8, Khaleq K9
DOI:https://doi.org/10.17511/ijmrr.2025.i02.10
1 Ettaoussi Abdelhak, Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, Morocco.
2 Jamaleddine Khalid, Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, Morocco.
3* Elhaddadi Mosaab, Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, Morocco.
4 Kamal Khadija, Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, Morocco.
5 Majd Abdessamad, Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, Morocco.
6 Bouali Mounir, Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, Morocco.
7 Elbakouri Abdelilah, Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, Morocco.
8 Elhattabi Khalid, Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, Morocco.
9 Khalid Khaleq, Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, Morocco.
Introduction: Peutz-Jeghers syndrome (PJS) is a rare autosomal dominant congenital disorder characterised by the presence of hamartomatous polyps in the gastrointestinal tract and mucocutaneous lentiginosis. It is associated with an elevated risk of cancer and substantial morbidity related to polyps, notably intestinal intussusception during childhood.
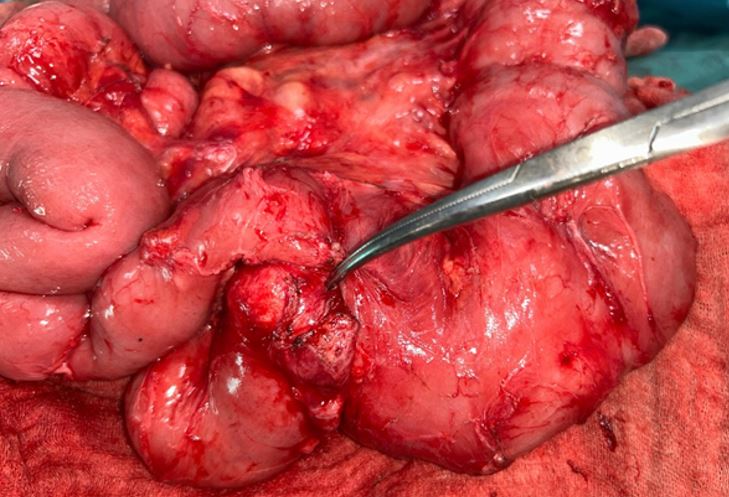
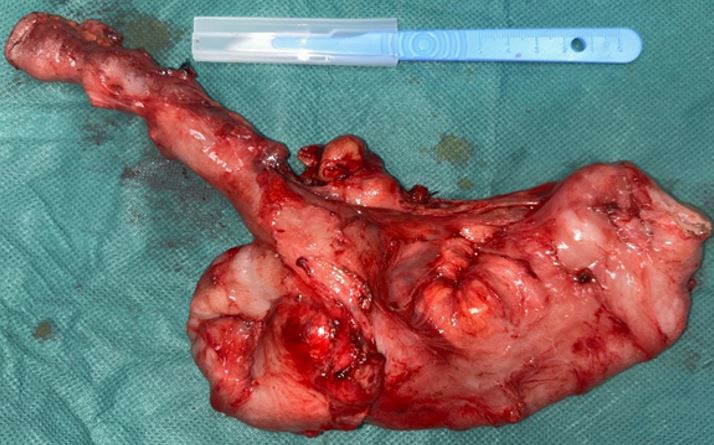
Case report: We report the case of a 32-year-old man patient, who consulted for subocclusif syndrome with multiple pigmented spots on the face and lips. Abdominal computed tomography (CT) revealed an image of jejuno-jejunal intussusception and substenotic jejunal mass. The patient underwent a double-segmental small bowel resection, removing the intussusception and the jejunal mass. The pathologic examination confirmed the diagnosis of Peutz-Jeghers polyps with moderately differentiated, invasive adenocarcinoma.
Discussion: The diagnosis of SPJ can be established in patients presenting one or more polyps and at least two of the associated clinical criteria: labial melanin deposits, family history of the syndrome and polyposis of the small bowel. Half of the cases present with small bowel obstruction. PJS is associated with an increased risk of gastrointestinal and non-gastrointestinal malignancies. Endoscopic or surgical polypectomy remains the preferred treatment option to prevent complications.
Conclusion: Regular surveillance of the gastrointestinal tract is recommended both for cancer prevention and early detection, and to prevent polyp-related complications, and certainly improve prognosis in these patients.
Keywords: Peutz-Jeghers syndrome, Hamartomatous polyp, Intussusception, Small bowel obstruction
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Medicine and Pharmacy of Casablanca, Visceral Emergency Department P35, IBN ROCHD University hospital of Casablanca, Casablanca, , Morocco. Email:  |
Abdelhak E, Khalid J, Mosaab E, Khadija K, Abdessamad M, Mounir B, Abdelilah E, Khalid E, Khaleq K, Small bowel obstruction in Peutz-Jeghers syndrome: case report. Int J Med Res Rev. 2025;13(2):46-51. Available From https://ijmrr.medresearch.in/index.php/ijmrr/article/view/1551 |
 |
 ©
©